Investigating stress response to a social evaluative threat in female and male children with Autism Spectrum Disorder
ABSTRACT
Autism spectrum disorder (ASD) is a condition that impairs social ability, and is more frequently diagnosed in males than females. A proven method of testing abnormalities in social behavior is by measuring stress response to a controlled social evaluative threat like the Trier Social Stress Test (TSST). While previous results have shown that male children with ASD have a lower stress response to the paradigm than typically developing (TD) males, comparable studies of female children are limited due to a lack of ASD diagnoses in females. This study is the result of increased efforts to collect more female data. A comparison was performed using the TSST to measure differences between males and females with ASD. Results showed that there was no significant difference found between stress responses in males and females with ASD, and there was a moderate correlation between communication deficits and having a lower stress response. This indicates that males and females with ASD have similar stress responses, and lesser communication skills correlate with atypical stress responses to social evaluative threats within the ASD group. This research will be utilized to make future comparisons between TD children and children with ASD, and provides more female representation in ASD research.
INTRODUCTION.
Autism spectrum disorder (ASD) is a developmental disorder that impairs social behavior and communication. In 2018, the CDC reported that this condition affects about 1 in 59 8-year old children [1]. Since the exact cause of the disorder is unknown, behavioral and physiological measures are utilized to understand more about ASD [2, 3, 4]. One aspect of ASD that warrants further research is how it affects children in socially stressful conditions, behaviorally and biologically. Testing the way an individual responds to stressful situations is a good method of finding and analyzing social impairments. This marks the importance of studying typically developing (TD) children in comparison to children with ASD in regards to stress response.
Recent ASD research has focused on the behavioral and hormonal responses of ASD adolescents to social stress. A reliable way to measure stress is by measuring cortisol, which is a hormone produced by the endocrine system that causes a feeling of anxiety and stress. The Trier Social Stress Test (TSST) is an effective and flexible model for measuring stress response because it puts participants in a socially stressful situation and provides intervals when salivary cortisol can be measured [5, 6, 7, 8]. The adaptive, typical response to the TSST is elevated cortisol. Previous work by Edmiston et al. (2017) used salivary cortisol levels to show that the stress response range of ASD adolescent males is more blunted than that of TD adolescent males due to the ASD group having an abnormal response to the TSST. One limitation of this research is the limited number of females included due to the gender imbalance of ASD diagnoses [7, 3]. The APA reports a 4 to 1 ratio of ASD diagnoses among males to females, making it challenging to recruit females as participants in ASD studies, and the disorder is typically less noticeable in females, making diagnosis more challenging [9, 10]. The combination of these factors often leads to researchers omitting female data due to an inability to fully compare it to male data [7].
Thus, this study aimed to compare the stress responses of children with ASD to the TSST by sex, using salivary cortisol as a measurement of stress response. TD data was used as a control to compare data from the ASD group. Based on previous findings, children with ASD were expected to have blunted cortisol responses compared to TD children [7, 8]. Female children with ASD were expected to have similar overall cortisol stress responses to males with ASD, but to have more variable cortisol at peaks and baseline measurements, as stated in previous research comparing males and female serum cortisol response to a blood draw stressor [11]. Higher cortisol was expected from more high-functioning participants with ASD and TD participants.
MATERIALS AND METHODS.
Ninety children with ASD (64 males, 26 females) and 66 TD children (41 males, 25 females) from ages 10-13 were included in the study. Participants were from the mid-south region of the U.S., the majority from Tennessee. Before evaluation, all participants and their parents or legal guardians were given informed consent forms to review and sign. IQ and age did not significantly differ between participants, shown by a Levene’s Test for Equality of Variances (Age: P = 0.98, F = 0.001; IQ: P = 0.70, F = 0.148). 6 ASD males had missing data from the TSST and therefore could not be included in the cortisol data. Specific demographics are shown in Table 1.
Table 1. Averages of participant demographics
| N | Age | Full-scale IQ | SCQ Total | SRS-2 Total T-score | ADOS-2 Comparison | |
| Male (ASD) | 70 | 11.32 | 101.84 | 17.71 | 74.21 | 7.4 |
| Female (ASD) | 26** | 11.24 | 99.62 | 15.19 | 77.35 | 6.08 |
| Male (TD) | 41 | 11.36 | 121.59 | 2.85 | 45.49 | * |
| Female (TD) | 25 | 12.00 | 114.96 | 2.20 | 48.68 | * |
| * TD participants did not complete the ADOS-2 assessment.
** Only 25 participants for the ADOS-2 assessment. |
||||||
Prerequisite measures.
In order to determine participant eligibility and certain statistics that would define TD and ASD groups, a variety of diagnostic measures were given to all study subjects. These prerequisites were performed before the social stress test and were considered alongside medical statements and previous assessments of each participant.
Diagnostic measures.
WASI-II [12]: The Wechsler Abbreviated Scale of Intelligence, 2nd edition provides an estimate of participant IQ. Scores on this diagnostic coupled with overall ability to comprehend information and instructions were factored into the selection of eligible participants for this study.
ADOS-2 [13]: The Autism Diagnostic Observation Schedule, 2nd edition (ADOS-2) is an observational procedure that allows participants to be tested for autism following the DSM-IV criteria for an autism diagnosis. Participants with ASD included in the data scored at least a 7 on the ADOS-2 scale, with the exception of 4 female participants who were included on the basis of clinical diagnosis, history with autism, scores on the SRS-2 and SCQ, and other behavioral factors. Using this data did not impact any of the correlations found in this study, as no significant differences were found in the dataset when the 4 females were removed (p = 0.117).
Dependent measures.
SCQ [14]: The social communication questionnaire (SCQ) is a parent form inquiring about the prevalence of behaviors in their children indicative of autism, and supports a clinician and ADOS-2 diagnosis of autism. An SCQ score of 15 or higher signals ASD. All TD participants had an SCQ score lower than 10.
SRS-2 [15]: The SRS-2 is a questionnaire designed to show abnormalities in social behavior associated with ASD using 5 sub-categories: Social Awareness, Social Motivation, Social Cognition, Social Communication, and Restrictive and Repetitive Behaviors (RRB). Participants with ASD scored at least a 50 on this measure.
The Trier Social Stress Test.
The Trier Social Stress Test (TSST) exposes participants to a socially stressful situation designed to yield a significant stress response [6]. The TSST is often utilized to show how differently those with social impairments such as ASD interpret scenarios designed to be socially stressful [5, 7]. The participant was given instructions to prepare the ending of a story that would be judged by two raters. The participant was informed that they are in competition with other children, and their job was to make their ending as exciting as possible. The participant was given 5 minutes to prepare for this interaction, giving a cortisol sample during that time, and then 5 minutes to tell their story. They were then asked to do 5 minutes of serial math subtraction. Several cortisol samples were taken in 10 to 20 minute increments following this interaction, as shown in Figure 1.
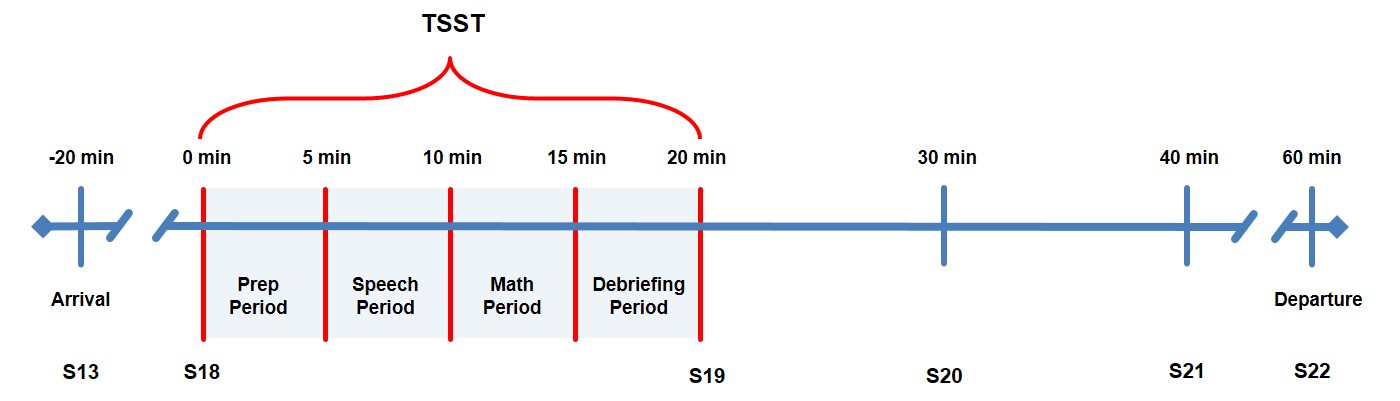
Figure 1. A timeline of the TSST procedures. Salivary cortisol samples (CS) were taken 20 minutes before the test after acclimating to their surroundings (CS13), right before the test (CS18), right after the test (CS19), in 10 minute increments after the test (CS20, CS21), and then at departure, which was 60 minutes after the test (CS22). Figure modified from Edmiston et al., 2017.
Cortisol sampling.
Salivary cortisol was sampled at home to obtain baseline measurements for 3 days prior to the TSST. Each day, two samples were taken in the morning, one was taken in the afternoon, and one was taken at night 30 minutes prior to bedtime, summing to a total of 12 samples. Participants were given Trident chewing gum to stimulate saliva production and saliva was collected by participants passively drooling into a tube. Samples were stored in the home refrigerator until the 4th day, when they were brought to the test site and stored at -20 ℃. Cortisol salivary assay procedure was performed on the samples using the methods described in previous research [7].
Statistics.
Between-group analyses of variance (ANOVAs) were run within TD and ASD groups between sexes using data collected from the demographics and log-transformed mean cortisol levels. Pearson correlations were used to test for correlations between cortisol samples, demographic factors, and sex. Levene’s Test for Equal Variances, a statistical analysis method that indicates difference in variance within a dataset, was used when comparing sex differences between ASD and TD groups. Statistical analyses were conducted using the alpha level (p = 0.05).
RESULTS.
In order to determine the differences between males and females within the ASD group, stress responses to the TSST and results from prerequisite measures were compared. There was no significant difference in cortisol between sexes within the ASD group for each stage of the TSST (Figure 2), as confirmed by the Levene’s Test for Equality of Variances (F = 0.66, p = 0.4).
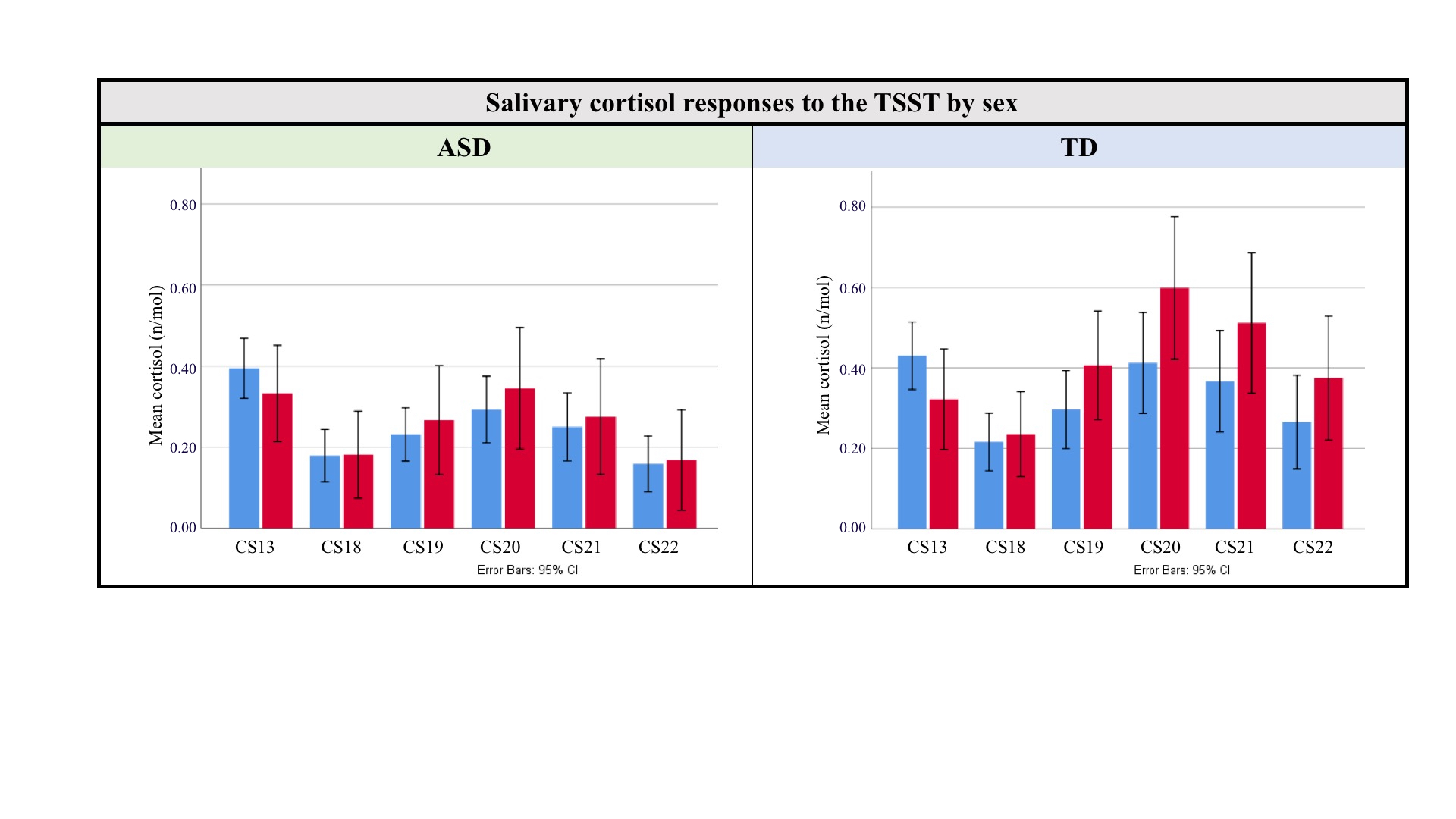
Figure 2: ASD and TD salivary cortisol responses to the TSST by sex. Levene’s Test for Equality of Variances done on variability between males (blue) and females (red) on the ASD group, and no significant variability was found (p = 0.4).
Age was shown to correlate positively with log-transformed mean cortisol from Cortisol Sample 20 (CS20) in the TSST (r = 0.21, p = 0.05). SRS-2 RRB t-scores from the group correlated negatively with Cortisol Sample 21 (CS21) mean cortisol, (r = -0.23, p = 0.03) such that a higher age was correlated with a more typical stress response (higher cortisol), and more RRBs were correlated with less of a typical stress response (lower cortisol). This data supports that there could be significant correlation between age and stress and repeated and repetitive behaviors and stress in children with ASD. Additionally, the data revealed a moderate inverse correlation between cortisol means and average communication t-score on the SRS-2, such that higher cortisol was correlated with lower SRS-communication scores in 3 mean cortisol samples (CS20, CS21, CS22), as shown in Figure 3 (CS20: r = -0.2, p = 0. 06; CS21: r = -0.23, p = 0.03; r = -0.20, p = 0.05). This indicates a more typical stress response from participants with ASD who had better communication skills according to the SRS-2.
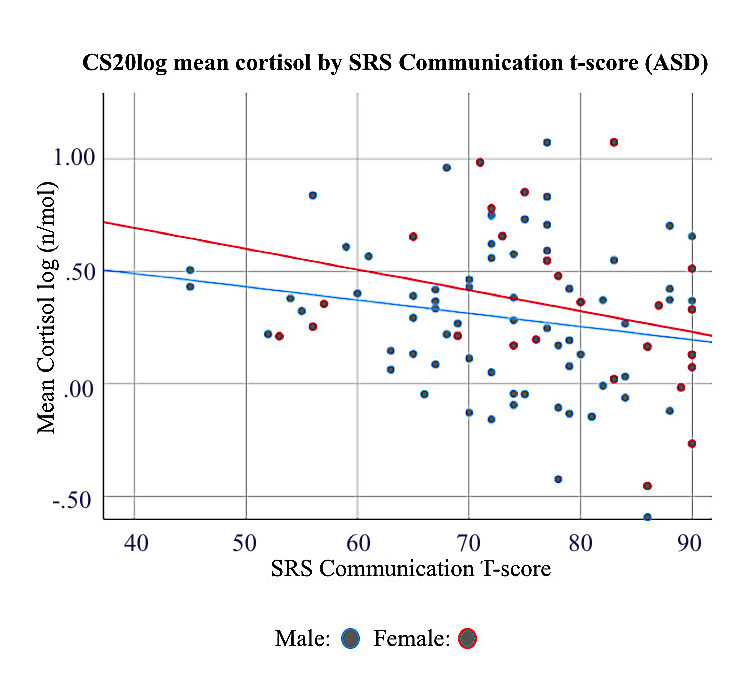
Figure 3. SRS-2 communication t-scores from ASD male and female children compared to mean cortisol response to the TSST. Females had a stronger negative correlation than males (Male R2 linear = 0.035, Female R2 linear = 0.08).
DISCUSSION.
This study investigated the differences in stress response between males and females with ASD, and found correlations between stress response and other social communication factors. The data suggests blunted cortisol response to the TSST in children with ASD compared to TD children. This finding is supported by the previous literature [7, 8]. Currently, the direct statistical comparison between the ASD and TD groups are the subject of another, ongoing study. However, it can be inferred within this study that the addition of females into the data pool did not significantly change the comparison of TD and ASD stress responses, in contrast to predictions stating the addition of females would alter these comparisons.
There was no significant difference in stress response between sexes, indicating that females and males with ASD have similar reactions to social evaluative threats. While female data appeared to have more variations due to large error bars, statistical analysis showed that there were no significant changes in variability between sexes, highlighting more similarities between males and females. A probable explanation for these large error bars in the female group stems from the limited number of females that were included in this study, despite increased efforts to overcome the 4:1 male to female diagnosis ratio. This finding contrasts previous research suggesting higher variability of stress response in females and males [11]. Future research warrants the inclusion of more female participants, both TD and with ASD, to make a reasoned conclusion.
Additionally, there was a moderate inverse correlation between SRS-2 communication t-scores and cortisol response to the TSST, meaning that as the reported ability to communicate increased, cortisol decreased. This correlation was only seen among the ASD participants, and was stronger in females (r = -0.21) than in males (r = -0.13). This data suggests that, within the ASD group, those with better parent-reported communication skills have a more typical stress response to social evaluative threats than those with less communicative ability. This finding is supported by additional research, which states high-functioning people with have more typical responses to social situations than those who have more severe social impairments [16].
There were also other correlations between age and cortisol and RRB and cortisol. According to this data, higher age was correlated with higher stress responses, and RRB (indicative of autism) was correlated with a less typical stress response. The latter correlation supports the major correlation between SRS communication t-scores and cortisol because it indicates more social awareness as autism severity decreases within the ASD group. Additionally, previous research has shown that increased age correlates with more social awareness, which supports the positive correlation between age and cortisol [17]. However, due to a small sample size and inconsistencies found within cortisol samples, these correlations cannot be verified within this study, and warrant further research.
Despite rigorous study methods, this study had limitations. Due to the small number of females diagnosed with ASD, the study had an imbalance of males and females. This may have reduced ability to accurately compare male and female groups. Additionally, the age range of participants was somewhat restricted given the participants needed to be 10-13 years old for the standardization of results.
CONCLUSION.
The results of this study suggest that there is no difference between female and male stress responses in children with ASD, and that there is a correlation between communication deficits and stress response in children with ASD. Future directions include comparing TD and ASD groups, analyzing data from multiple years of the pubertal development, and continuing to collect data from females. These results highlight the importance of researching differences in behavior by sex in adolescents with ASD, and are important for the treatment and future diagnoses of people with ASD.
ACKNOWLEDGMENTS.
The authors would like to thank the participation of the families involved in this study. The research for this study was funded by NIMH R01 MH085717. The authors have no conflicts of interest to declare.
REFERENCES.
- Centers for Disease Control and Prevention. ADDM Community Report on Autism 2018 (2018).
- Kogan, M. D., Blumberg, S. J., Schieve, L. A., Boyle, C. A., Perrin, J. M., Gandhour, R. M., . . . Van Dyck, P. C. Prevalence of Parent-Reported Diagnosis of Autism Spectrum Disorder Among Children in the US, 2007. Pediatrics 124, 1395-1403 (2009).
- Edmiston, E. K., Jones R. M., and Corbett, B. A. Physiological Response to Social Evaluative Threat in Adolescents with Autism Spectrum Disorder. Journal of Autism and Developmental Disorders 46, 2992–3005 (2016).
- Jansen L. M. C., Gispen-de Wied C. C., van der Gaag R. J., van Engeland H. Differentiation between autism and multiple complex developmental disorder in response to psychosocial stress. Neuropsychopharmacology 28, 582–590 (2003).
- Allen AP, Kennedy PJ, Dockray S, Cryan JF, Dinan TG, Clarke G. The Trier Social Stress Test: Principles and practice. Neurobiol Stress. 12, 113-126 (2016).
- Kirschbaum, C., Pirke, K. M., & Hellhammer, D. H. The ‘Trier Social Stress Test’—a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology 28, 76–81 (1993).
- Edmiston, E. K., Blain, S. D. and Corbett, B. A. Salivary cortisol and behavioral response to social evaluative threat in adolescents with autism spectrum disorder. Autism Research 10, 346–358 (2017).
- Lanni KE, Schupp CW, Simon D, Corbett BA. Verbal ability, social stress, and anxiety in children with Autistic Disorder. Autism. 16 123–138 (2012).
- APA. Diagnostic and statistical manual of mental disorders, fifth edition (DSM-5). Washington, DC: American Psychiatric Association (2013).
- Dean, M., Harwood, R., & Kasari, C. The art of camouflage: Gender differences in the social behaviors of girls and boys with autism spectrum disorder. SAGE Journals 21, 678-689 (2016).
- Spratt, E. G., Nicholas, J. S., Brady, K. T., Carpenter, L. A., Hatcher, C. R., Meekins, K. A. Charles, J. M. Enhanced Cortisol Response to Stress in Children in Autism. Journal for Autism and Developmental Disorders 42, 75-81 (2012).
- Wechsler, D. Wechsler Abbreviated Scale of Intelligence. San Antonio, TX: Psychological Corporation (1999).
- Lord, C., Rutter, M., DiLavore, P.S., Risi, S. Autism Diagnostic Observation Schedule (ADOS). Los Angeles, CA: Western Psychological Services (1999).
- Rutter, M., Bailey, A., and Lord, C. The Social Communication Questionnaire: Manual. Los Angeles, CA: Western Psychological Services (2003).
- Constantino, J.N., & Gruber, C.P. Social responsiveness scale. Los Angeles: Western Psychological Services (2012).
- Ben-Itzchak, E., & Zachor, D. A. The effects of intellectual functioning and autism severity on outcome of early behavioral intervention for children with autism. Research in Developmental Disabilities28, 287–303 (2007).
- Seltzer, M. M., Shattuck, P., Abbeduto, L., & Greenberg, J. S. Trajectory of development in adolescents and adults with autism. Mental Retardation and Developmental Disabilities Research Reviews10, 234–247 (2005).
Posted by John Lee on Wednesday, December 23, 2020 in May 2020.